X
Subscribe!
Get the latest updates on SmartMan!
Subscribe!
Get the latest updates on SmartMan!
Click HERE for PDF
To download copy of the guidelines go here: https://www.erc.edu/index.php/publications_home/en/ and select the part that you want.
The Section that applies is “Feedback on compression technique” in Section 1, page 11
References referred to in the above section are:
99. Cooper K, Salman B, Soar J, Finn J, Perkins GD. Debriefing to improve outcomes from critical illness: a systematic review and meta-analysis. Intensive Care Med 2013;39:1513-23
100. Couper K, Kimani PK, Abella BS, et al. The system-wide effect of real-time audiovisual feedback and postevent debriefing for in-hospital cardiac arrest: the cardiopulmonary resuscitation quality improvement initiative. Crit Care Med 2015 [in press]
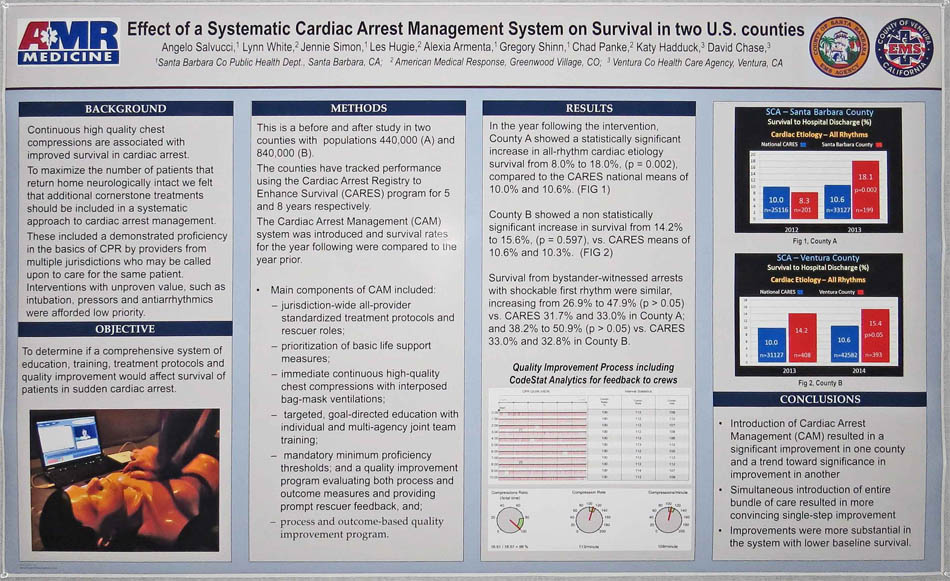
EFFECT OF A SYSTEMATIC CARDIAC ARREST MANAGEMENT SYSTEM ON SURVIVAL IN TWO US COUNTIES
Angelo Salvucci1, Lynn White2, Jennie Simon1, Les Hugie2, Alexia Armenta1, Gregory Shinn1, Chad Panke2, Katy Hadduck3, David Chase3, 1Santa Barbara County Public Health Department, Santa Barbara, California, USA, 2American Medical Response, Greenwood Village, Colorado, USA, 3Ventura County Health Care Agency, Ventura, California, USA
Objective: To evaluate the survival effect of the addition of a cardiac arrest management (CAM) system in two US counties.
Methods: This is a before and after study in two counties; populations 440,000 (A) and 840,000 (B). The counties have tracked performance using the Cardiac Arrest Registry to Enhance Survival (CARES) program for 5 and 8 years respectively. The CAM system was introduced and survival rates for the year following were compared to the year prior. Main components of CAM included: jurisdiction-wide all-provider standardized treatment protocols and rescuer roles; prioritization of basic life support measures; immediate continuous high-quality chest compressions with interposed bag-mask ventilations; targeted, goal-directed education with individual and multi-agency joint team training and mandatory minimum proficiency thresholds; and a quality improvement program evaluating both process and outcome measures and providing prompt rescuer feedback.
Results: In the year following the intervention, County A showed a statistically significant increase in all-rhythm cardiac-etiology survival from 8.0% to 18.0%, (p = 0.002), compared to the CARES national means of 10.0% and 10.6%. County B showed a non-statistically significant increase in survival from 14.2% to 15.6%, (p = 0.597), vs. CARES means of 10.6% and 10.3%. Survival from bystander-witnessed arrests with shockable first rhythm were similar, increasing from 26.9% to 47.9% (p > 0.05) vs. CARES 31.7% and 33.0% in County A and 38.2% to 50.9% (p > 0.05) vs. CARES 33.0% and 32.8% in County B.
Conclusion: The addition of the Cardiac Arrest Management system was associated with increases in survival rates in both communities. County A, which began with a survival rate below the national CARES mean, showed a profound and statistically significant survival improvement in the year following the system’s introduction. County B began with a survival rate above the CARES national mean, and showed a non-significant increase in survival.
SmartMan is a private company creating training systems to improve survival rates. We also provide consultation and guidance on implementing system wide solutions.
Theme by CssTemplateHeaven